Messaging Guide
Ankle Plating System 3
Evidence
Why This Matters
This retrospective study examined the rate of syndesmotic instability following direct reduction and stabilization of the posterior malleolus compared to the rate of instability for those treated conservatively. Of the patients who underwent direct posterior malleolar fixation, 97.9% achieved syndesmotic stability without additional syndesmotic fixation. Acumed was first to market with precontoured posterior malleolar plates designed to aid the surgeon in fracture reduction while reducing the need for intraoperative bending.
Publication Excerpt
“Our data demonstrates that the rate of syndesmotic instability was reduced in trimalleolar and trimalleolar equivalent fractures when prone positioning and direct fixation of the posterior malleolus were first performed.”
The First Fragment-Specific Posterior Distal Tibia Plates on the Market
With 67% of posterior malleolus fractures involving the lateral corner,1 Acumed oers fragment-specific plates contoured to fit each side of the posterior malleolus and to capture comminution at the articular surface.
Thin Lateral Fibula Plates
Designed to minimize soft tissue irritation, these plates are thinner both distally and proximally than DePuy Synthes, Arthrex, and Zimmer Biomet lateral fibula plates.2
Two Styles of Hook Plates
These plates can be placed on either the lateral or medial malleolus. The Locking Peg Hook Plate includes a 2.3 mm Locking Cortical Peg across the fracture for added support, and the fracture can be compressed and held in place during surgery with the Hook Plate Reduction Handle.
Two Plates, One Incision
A single incision is possible for both the Posterolateral Fibula and Posterolateral Distal Tibia plates to address a trimalleolar ankle fracture.

1. Haraguchi N, Haruyama H, Toga H, Kato F. et al. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006;88:1085-1092.
2. Internal document on file.
Small Fragment Base Set
Origin Story
Compared with competitor small fragment products, which often include only the basic plates and instrumentation needed for plate implantation, the Acumed Small Fragment Base Set provides a comprehensive system. In addition to including the standard components, we provide 2.7 mm Fragment Plates that can be used on small bones and updated instrumentation designed to streamline the surgical experience and reduce the time spent on each case.
Comprehensive System
Designed for small fragment trauma surgeries of the upper and lower extremities, the set can be used as both a stand-alone system and in conjunction with Acumed’s Ankle Plating System 3.
A Choice of Plates
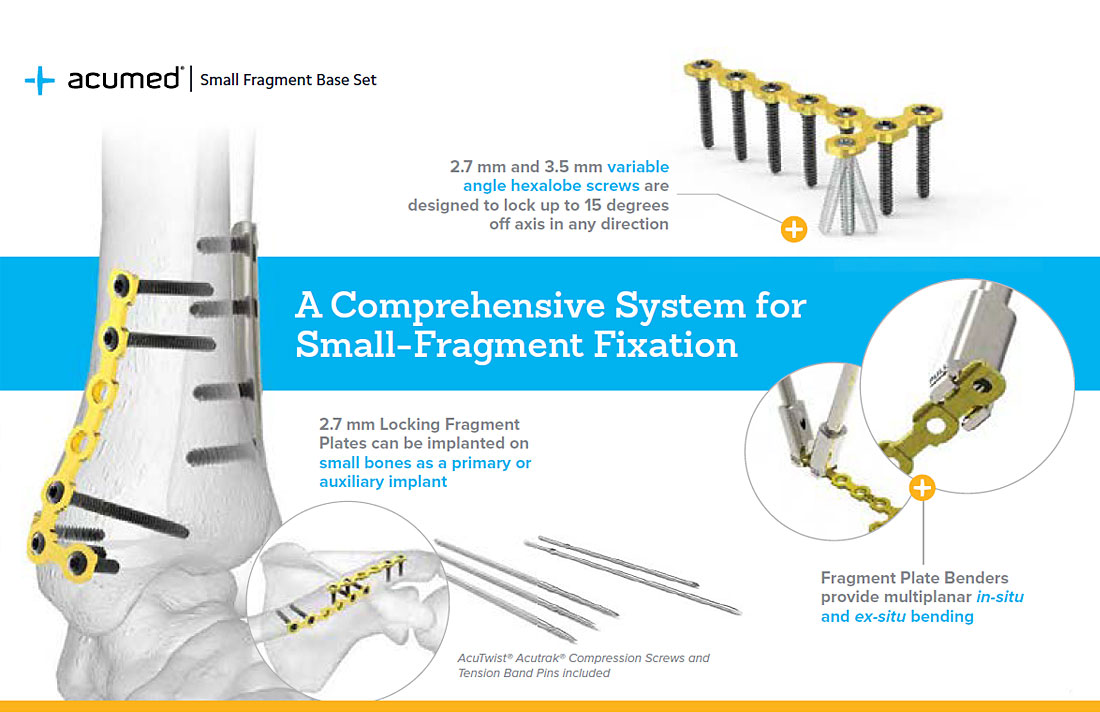
The Small Fragment Base Set includes nonlocking One-Third Tubular Plates that can be used on the clavicle, scapula, olecranon, humerus, radius, ulna, distal tibia, and fibula. The 2.7 mm Locking Fragment Plates can be implanted on small bones as a primary or auxiliary implant.
Plate Benders
Fragment Plate Benders allow for in-situ and ex-situ bending in a multiplanar direction and may be slid over a plate hole with an existing screw.
Additional Implants
The Small Fragment Base Set also houses three lengths of nonsterile AcuTwist® Acutrak® Compression Screws and Tension Band Pins to facilitate fracture reduction, providing several implant options to support the case.
Variable Angle Screws
These screws are designed to lock up to 15 degrees off axis in any direction, allowing the surgeon to target the best quality bone and avoid joint penetration.
Fibula Rod System
Evidence
Why This Matters
Comorbidities and implant prominence are problematic for elderly patient populations presenting with ankle fractures. With a minimally invasive approach and reduced hardware prominence, fibular nailing provides an alternative to open reduction internal fixation (ORIF) while reducing the need for secondary hardware removal.
Publication Excerpt
“The fibula nail provides an alternative to standard plate fixation that uses a minimal approach and, therefore, decreases the incidence of wound infection and the need for further surgery to remove prominent metalwork while providing stable fixation.”
Minimally Invasive
The nail is inserted in the distal fibula through a minimal incision. Screws are inserted by making stab incisions to protect the soft tissue envelope and preserve vascularity of the periosteum.
Precontoured Design
The nail has a five-degree bend designed to fit the intramedullary canal of the fibula.
Streamlined Procedure
The surgical technique consists of eight steps from start to finish, streamlining valuable surgery time.
Targeting Guide
The targeting guide aids in the correct placement of both A/P and L/M screws and allows for syndesmotic screw fixation.

Acutrak 2® Headless Compression Screw System
Evidence
Why This Matters
For the treatment of symptomatic subtalar arthrodesis, excessive relative motion between the talus and calcaneus can delay or prohibit fusion. This study quantifies the torsional resistance of 2-screw and 3-screw subtalar joint fixation. In this study, performance of the Acutrak screws exceeded that of conventional lag screws regardless of whether two or three Acutrak screws were used.
Publication Excerpt
“Performance of the tapered, fully threaded, variable pitch screws exceeded that of conventional lag screws regardless of whether two or three screws were used. Additional resistance to internal rotation afforded by a third screw placed anteriorly may offer some advantage in patients at risk for nonunion.”
A Comprehensive Solution
The Acutrak 2 Headless Compression Screw system is available in six dierent families for a total of 68 dierent screws to address a variety of foot and ankle applications.
Lateral Malleolus Fixation
A clinical study showed the fully threaded, continuously variable Acutrak thread pitch provides compression and aids in rotational stability of the fibula.2
A Larger “Window of Compression”
Acutrak technology has a wide window of compression, which is less sensitive to loss of compression due to stripping the bone and is more flexible in its placement depth, enabling a maximum amount of compression.3
2. Lee YS, Hsu TL, Huang CR, Chen SH. Lateral fixation of AO type-B2 ankle fractures: the Acutrak Plus compression screw technique. Int Orthop. 2010;34(6):903-907.
3. Wheeler DL, McLoughlin SW. Biomechanical assessment of compression screws. Clin Orthop Relat Res. 1998;350:237–245.

Calcaneal Plating System
Evidence
Why This Matters
Acumed MINI-Calc plates were deigned to be implanted via a sinus tarsi approach that limits the size of the operative incision. This study compared the sinus tarsi and extensile approaches, finding that the rate of wound complication was 3.6% in the sinus taris group versus 13.5% for the extensile approach group. With no statistical significance in AOFAS and VAS scores, the sinus tarsi approach may be favorable for reducing postoperative complications.
Publication Excerpt
“Limited open reduction via the sinus tarsi approach for intra-articular calcaneal fractures could reduce the incidence of wound complications effectively, and the medial distraction technique is helpful for correcting the calcaneus varus deformity.”
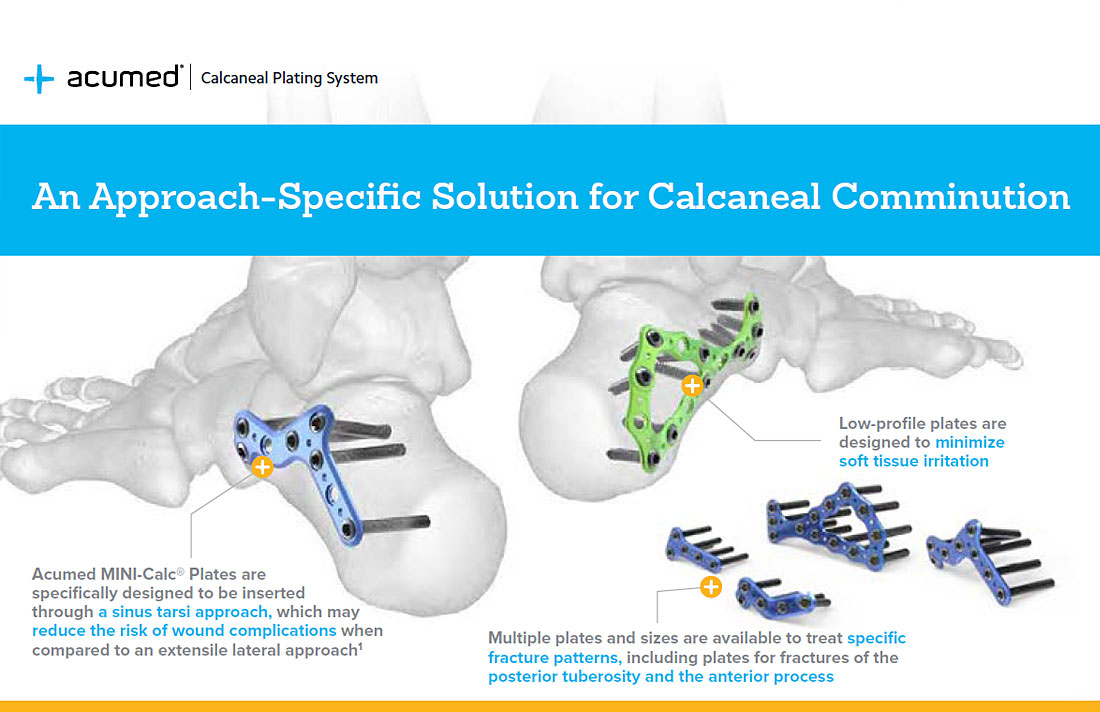
Plates Designed Specifically for a Sinus Tarsi Approach
MINI-Calc® Plates offer a variety of plate options in a low-profile design and can be used through a sinus tarsi approach for minimally invasive treatment.
Fragment-Specific Options
Whether comminution is present in the anterior process, through the posterior facet, in the anterior tuberosity, or any combination, multiple plates and sizes are available to treat each of these fracture patterns.
Low-Profile Plates
The MINI-Calc Plates are 1.25 mm thick and are designed to minimize soft tissue irritation.
1. Haraguchi N, Haruyama H, Toga H, Kato F. et al. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am. 2006;88:1085-92.
2. Internal document on file.